UUnderweight is reportedly becoming increasingly common among young women. A phenomenon specific to Japan and not seen in other developed countries, it is a problem because of its close relationship to the risk of having a low birthweight infant —— that is to say, expectant mothers who are underweight are more prone to preterm delivery and delivering low birthweight infants. It has also emerged that adults who were born with low birthweight are more prone to lifestyle-related diseases such as obesity, cardiovascular diseases, and type 2 diabetes. Healthy physical status of the mother is very important, as it affects her child’s future, and begins with her nutritional management even before pregnancy.
Special Feature 1 – Children’s Nutrition Maternal nutrition in pregnancy affects future health
composition by Yumi Ohuchi

Hidemi Takimoto
Chief, Department of Nutritional Epidemiology and Shokuiku, National Institute of Health and Nutrition, National Institutes of Biomedical Innovation, Health and Nutrition
Graduated from the School of Medicine at Tokyo Medical and Dental University's Faculty of Medicine in 1991. Joined the National Institute of Health and Nutrition as a research fellow in the Section of Maternal and Child Health in September 1994. After becoming Chief of the Section of Maternal and Child Health in the Department of Health Promotion, National Institute of Public Health in 2005, she took up concurrent positions in 2012 as Chief of the Department of Nutritional Education and Chief of the Department of Nutritional Epidemiology at the National Institute of Health and Nutrition (now part of the National Institutes of Biomedical Innovation, Health and Nutrition). Dr. Takimoto has held her current post since 2017. Dr. Takimoto was involved in research for drafting the 2021 revision of the Dietary Guidelines for Pregnant and Lactating Women.
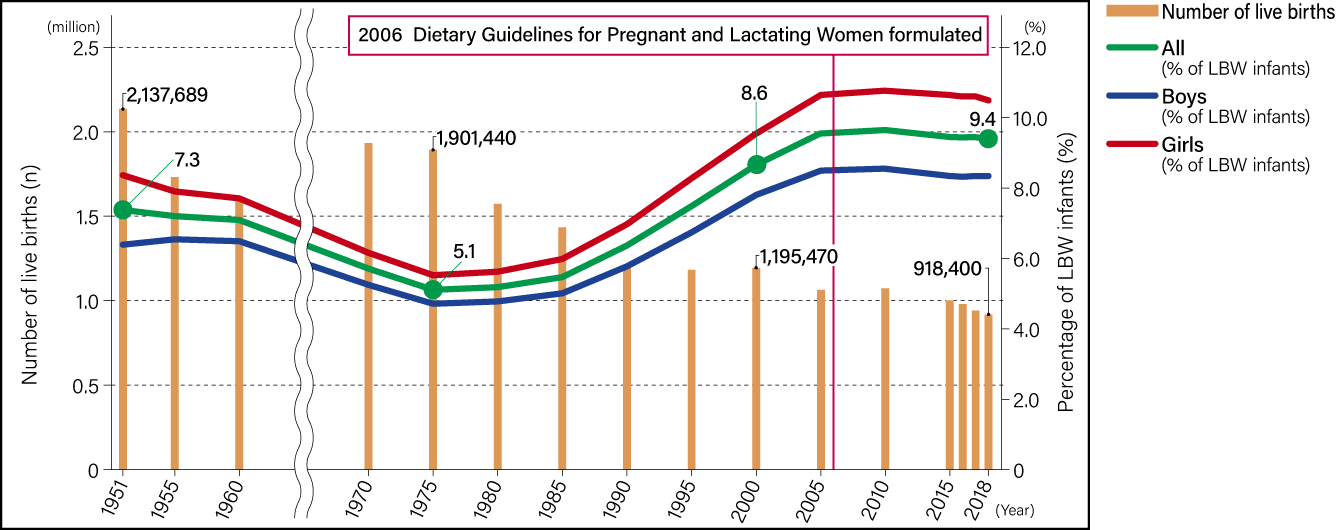
Japan currently has very low rates of both maternal mortality (3.3 per 100,000 total births) and infant mortality under 1 year old (1.9 per 1,000 live births), demonstrating the excellence of Japanese medical care for mothers and children (Vital Statistics of Japan 2019). However, at the same time, declining birthweights and an increase in the number of low birthweight (LBW) infants (those weighing less than 2,500 g) are becoming a problem. After peaking in the mid-1970s, mean birthweight fell until around 2005, since then they have remained more or less stable. After experiencing its biggest fall in the mid-1970s, the proportion of LBW infants saw a linear increase until 2004, since when the trend has remained flat. More shockingly, the prevalence of LBW infants is increasing to such an extent that mean birthweight is lower in this modern age of dietary abundance than they were in 1951, shortly after the end of World War II, when food supply was short (Figure 1).
 Compiled from data in Ministry of Health, Labour and Welfare, 2018 Vital Statistics of Japan
Compiled from data in Ministry of Health, Labour and Welfare, 2018 Vital Statistics of Japan
Figure 1. Number of live births and prevalence of LBW infants (<2500 g) (1951-2018)The number of live births halved between 1951 and 2018. While the proportion of LBW infants declined between 1951 and the 1970s, the figure rebounded thereafter, with no major change over the last 10 years or so.
Looking at the situation worldwide, the proportion of LBW infants is, at 9.4%, higher than the average of 6.6% among countries belonging to the Organisation for Economic Co-operation and Development (OECD). Also problematic is the fact that, given Japan’s proportion of preterm deliveries is 5.7% and therefore lower than the OECD average of 7.9%, the majority of LBW infants is not due to preterm delivery.
Underweight increases the risk of having a LBW infant
Many studies have revealed the possibility of an increased risk of developing lifestyle-related diseases such as obesity, cardiovascular diseases, and type 2 diabetes in adulthood among those whose prenatal development was inadequate, such as preterm delivery and LBW. This phenomenon is called the Developmental Origins of Health and Disease (DOHaD) hypothesis. Given that the proportion of LBW infants is stable at almost 10%, this means one child in 10 is potentially born at risk of developing lifestyle-related diseases in the future.
Furthermore, in recent years, many studies have shown that the impact of weight gain on fetal development differs according to the individual’s pre-pregnancy nutritional status, with a stronger effect seen in the case of underweight women, leading to an increased risk of perinatal abnormalities such as preterm delivery and LBW. Looking at the nutritional status of young Japanese women, the 2017 National Health and Nutrition Survey showed that the proportion who were underweight (BMI<18.5) has crept up from 15.1% of women in their 20s and 7.2% of those in their 30s in 1973 to 21.7% and 13.4% respectively in 2017 (Figure 2). The same trend emerged —— albeit with slightly older data covering the period from 1976 to 2000 —— in an article my colleagues and I published in 2004, suggesting that underweight among young women has increased nationwide.
- * Thinness among young Japanese women
H Takimoto, N Yoshiike, F Kaneda, K Yoshita – American journal of public health, 2004
 Compiled from data in Ministry of Health, Labour and Welfare, 2017 National Health and Nutrition Survey
Compiled from data in Ministry of Health, Labour and Welfare, 2017 National Health and Nutrition Survey
Figure 2. Status of women’s weight and associated issuesThe proportion of underweight (BMI<18.5) individuals was 15.1% in the 20-29 age bracket and 7.2% in the 30-39 bracket in 1973, but has been on the rise since then.
Japan’s increase in underweight is an anomalous phenomenon when compared against similarly developed countries in the West, where the sharp rise in obesity is a major issue. While the reasons behind the situation are unknown, there is certainly a possibility that the increase in underweight among young women is influencing the rise in the prevalence of LBW infants.
Against this background, the Dietary Guidelines for Pregnant and Lactating Women formulated in 2006 were revised in 2021 for the first time in 15 years. Whereas the original guidelines had been formulated with a view to achieving a good diet during pregnancy and breastfeeding, the revised guidelines extended the focus to pre-pregnant women as well and were renamed Dietary Guidelines for Pre-pregnant, Pregnant and Lactating Women in Japan to reflect this change. Another major change was the advice regarding the amount of weight gain during pregnancy.
As gaining too much weight during pregnancy increases the risk of pregnancy-induced hypertension, gestational diabetes, and macrosomia, there was a time when pregnant women were advised to keep any weight gain to no more than 10 kg. Accordingly, many women might well have been instructed to avoid gaining much weight rather than to put it on. Reports on the incidence of gestational diabetes differ, varying from 4% to almost 10%. However, the majority of Japanese women with gestational diabetes are not obese, but are normal or even underweight, suggesting that the cause in such individuals is likely to be a lack of muscle mass or having insufficient insulin secretion.
In the 2006 Dietary Guidelines for Pregnant and Lactating Women, the recommended weight gain using pre-pregnancy nutritional status as the benchmark was set at 9-12 kg for underweight women (those with a BMI below 18.5) and 7-12 kg for women of normal weight (those with a BMI of 18.5 to 24.9). These figures were also mentioned in the Maternal and Child Health Handbook. Although the rise in the prevalence of LBW infants has been stemmed since then, there are no signs of a significant turnaround in the trend. Accordingly, the recent revision presented the Gestational Weight Gain Guidelines published in 2021 by the Japan Society of Obstetrics and Gynecology, and, using the pre-pregnancy nutritional status as a benchmark, set the weight gain range at 12-15 kg for underweight women and 10-13 kg for women of normal weight (Table 1). Based on comprehensive consideration of not only weight gains, but also pregnancy complications, using the latest data from sources such as the Neonatal Research Network Database in Japan, these figures have been calculated to be within a range that minimizes risk.
| Pre-pregnancy nutritional status*2 | BMI | Guidelines for weight gain guidance |
| Underweight | Less than 18.5 | 12-15 kg |
| Normal range | 18.5 to less than 25.0 | 10-13 kg |
| Obese (class I) |
25.0 to less than 30.0 | 7-10 kg |
| Obese (classes II & III) |
30.0 or more | Tailored individually (Up to a maximum of 5 kg as a guide) |
Table 1. Gestational weight gain guidelines*1The Dietary Guidelines for Pre-pregnant, Pregnant and Lactating Women in Japan set out the desirable level of weight gain in pregnancy, with reference to the Gestational Weight Gain Guidelines published by the Japan Society of Obstetrics and Gynecology.
*1 “Be aware that there is not necessarily sufficient evidence to justify stringent guidance regarding weight gain and take care to provide moderate guidance that takes individual differences into account” (From the Guideline for Gynecological Practice in Japan: Obstetrics Edition 2020, CQ 010)
*2 In accordance with the obesity classification used by the Japan Society for the Study of Obesity.
However, it should be noted that the figures do not constitute recommendations for weight gain targeted at pregnant women, but are rather a guide for health professionals who provide advice to pregnant women. Accordingly, the 2021 Dietary Guidelines encourage pregnant women to use these figures as a guide when checking their weight and to consult the medical personnel if they have any concerns. Moreover, another important point to note is that, as most women will achieve adequate fetal development in spite of less weight gain, and other cases in the opposite, medical personnel must be careful to provide advice based on each woman specifically.
The problem of malnutrition in young women
Weight is no more than a guide; it is the content of our diet that is important. As a result of reviewing data such as that from the 2017 National Health and Nutrition Survey in the course of revising the Dietary Guidelines, it became apparent that there are problems with diet even before pregnancy. For example, young women in their 20s and 30s are less likely than those in other age brackets to eat a balanced diet (meals composed of staple foods, main dishes, and side dishes). As many as 12% or so responded “rarely” when asked about the frequency with which they ate meals composed of staple foods, main dishes, and side dishes, whereas only around 40% (38.4% of women in their 20s and 42.8% of those in their 30s) stated that they ate such a diet “almost every day.”
Staple foods include such carbohydrate-rich items as rice, bread, and noodles, from which the body generates its energy. Comparing the average energy intake calculated from the National Health and Nutrition Survey with the estimated energy requirements prescribed in the Dietary Reference Intakes for Japanese (2015), we can see that such women are not consuming an adequate energy intake. In addition, whereas the target value for intake of vegetables, which are a source of vitamins and minerals, is 350 g per day [Health Japan 21 (the second term)], young women fell some way short of this figure, with those in their 20s consuming 218.4 g and those in their 30s 232.3 g on average.
Among those vitamins and minerals are folate and calcium, nutrients that are particularly important in pregnancy. A lack of folate in the early stages of pregnancy, when an intense process of cell division takes place, can potentially increase the risk of the fetus developing congenital abnormalities called neural tube defects. Neural tube defects are disorders caused by the failure of the neural tube that forms the brain and spinal cord to develop properly. These defects can cause motor and excretory disorders, as well as anencephaly, a condition in which brain tissue fails to develop, resulting in fetal death. Accordingly, not only those in the early stages of pregnancy, but everyone planning to become pregnant or who could possibly be pregnant is recommended to consume at least 400 µg of folic acid per day.
However, folate consumption among those in their 20s and 30s is lower than among older age groups and does not even reach the recommended level for those who are not pregnant. Fetal development during pregnancy and the secretion of breast milk after delivery leads to the mother’s body losing large quantities of calcium. Calcium intake by Japanese women in general is low and the lack of its adequate consumption has been an issue for many years.
Diet is not the only factor involved in ensuring a healthy body; exercise is important, too. Looking at the proportion of women who habitually exercise (at least two days each week for at least 30 minutes each time, continuing for at least a year) is almost 40% among those aged 65 or above, whereas the figure is lowest among women in their 20s (11.6%) and 30s (14.3%).
Thus, as shown above, many young women do not meet the recommended levels for energy and nutrient intake. However, in a survey (Report of the Committee Meeting on the Promotion of a Healthy and Sustainable Food Environment, 2021), 74.6% of underweight young women responded, “I do not wish to improve my diet.” Interestingly, looking at the sources of information influencing young women’s diets by physique, family have a major influence, with underweight young women reporting that family had the greatest influence, followed by television and websites.
From this, we can surmise that the influences of family and media are behind the underweight of young women today. Looking at the perspective of family in particular, children born since the 1970s, when underweight began to increase, are now old enough to be the mothers of today’s young women and might well have passed on dietary practices making them prone to underweight.
Underweight may not be a health problem if an individual’s physical activity level and intake of energy and nutrients are adequate, but those who are underweight due to low energy and nutrient intakes may need intervention. Given popular trends equating thinness with being more attractive, television, the internet, and other media must be used to proactively educate young women about the importance of building a healthy body, starting before pregnancy.
Furthermore, during pregnancy and breastfeeding, women need higher energy and nutrient intakes than before pregnancy, to ensure the healthy growth of both mother and baby. However, figures for average intakes of nutrients, etc. among pregnant women reported in the National Health and Nutrition Survey between 2015 and 2017 show that intake of numerous nutrients —— including vitamin A, D, B1, B2, B6, folate, vitamin C, calcium, magnesium, iron, and zinc —— was below the levels recommended or deemed adequate in the Dietary Reference Intakes for Japanese (2015). Intake of more than half of these nutrients did not even reach the levels recommended or deemed adequate for non-pregnant women, let alone the higher levels required in pregnancy. A survey of breastfeeding mothers also found that average intakes of energy, protein, and many vitamins and minerals were low (2017 National Health and Nutrition Survey). As changing one’s diet after becoming pregnant is not easy, it is preferable in light of this situation to ensure appropriate nutritional intakes from before pregnancy.
Consider nutritional balance, not only weight
The Dietary Guidelines for Pre-pregnant, Pregnant and Lactating Women in Japan set out 10 points regarding diet (Table 2) and provide specific explanations about elements regarding which women should be careful. However, it is not only efforts by the individual that are key to improving diet in pregnancy; individually tailored, appropriately timed interventions by medical institutions and government bodies, among others, are also important. In our research, we provided health guidance regarding weight gain to 406 healthy pregnant women and, where those women’s weight gain was above or below the benchmark at around 28 weeks of pregnancy, we had a dietitian provide them with nutritional guidance, to verify the effectiveness of dietary guidance interventions. The results showed a lower degree of excess or insufficient weight gain compared with the 28-week mark among subjects in the intervention group provided with individually tailored dietary advice than among the nonintervention group, and the percentage with excess or insufficient weight gain was also lower in the intervention group at the time of birth.
| (1) | Ingest a well-balanced diet before getting pregnant. |
|---|---|
| (2) | Achieve an adequate energy intake through staple foods. |
| (3) | Side dishes help you take in sufficient vitamins and minerals. |
| (4) | Optimize main dishes to increase intake of protein. |
| (5) | Dairy products, colored vegetables, beans, and small fish are good sources of calcium. |
| (6) | Adequate weight gain in pregnancy is ideal for you and your baby. |
| (7) | A well-balanced diet helps you breast feed. |
| (8) | Be physically active but avoid overdoing it. |
| (9) | Avoid smoking, passive smoking, and drinking alcohol. |
| (10) | Support from your family and friends helps you enjoy a healthy daily life with your baby. |
Table 2. 10 key points to ensure mother and baby can enjoy a healthy daily lifeThe Dietary Guidelines for Pre-pregnant, Pregnant and Lactating Women in Japan are published on the National Institute of Health and Nutrition website (https://www.nibiohn.go.jp/eiken/ninsanpu/). The Ministry of Health, Labour and Welfare website also has a leaflet with the Dietary Guidelines for Pre-pregnant, Pregnant and Lactating Women in Japan.
Additionally, as pregnancy and breastfeeding are times when women tend to experience instability in both their physical and mental conditions, kind-hearted support from family members and others around them is also crucial. But the most important thing for anyone who is pregnant or planning to become pregnant is to approach the creation of a healthy body in an enjoyable way that suits you, rather than worrying that you must do this or that.
For example, while consuming vitamins and minerals from eating enough vegetables is the ideal, I believe that taking dietary supplements in consultation with your physician is another option. Proper use of supplements is particularly advisable in the case of folate, where the bioavailability of food folate is lower. Using meal kits or delivery services can be an option for alleviating the burden of meal preparation. Rather than suppressing any worries or concerns, it is vital to seek support and advice, whether from your family and friends, a medical institution, a local maternal and child health center or group.
I want not only individuals, but also the whole of society to be aware of promoting the health of expectant and nursing mothers, regarding it as an issue that affects the very future of Japan.
(Figures courtesy of Hidemi Takimoto)